Understanding cerebral atrophy, a process often visualized through neuroimaging techniques like MRI, is critical in neurological assessments. Conditions such as hydrocephalus can sometimes mimic atrophy, leading to diagnostic complexities. This article explores the nuanced interpretation of mild to moderate ventriculomegaly is favored ex vacuo in nature, often observed on brain scans. Specifically, this is to differentiate true ventriculomegaly from the appearance of enlarged ventricles caused by surrounding cerebral volume loss. Radiologists play a crucial role in distinguishing these findings, considering the patient’s clinical history and employing volumetric analysis tools to aid in accurate diagnosis.
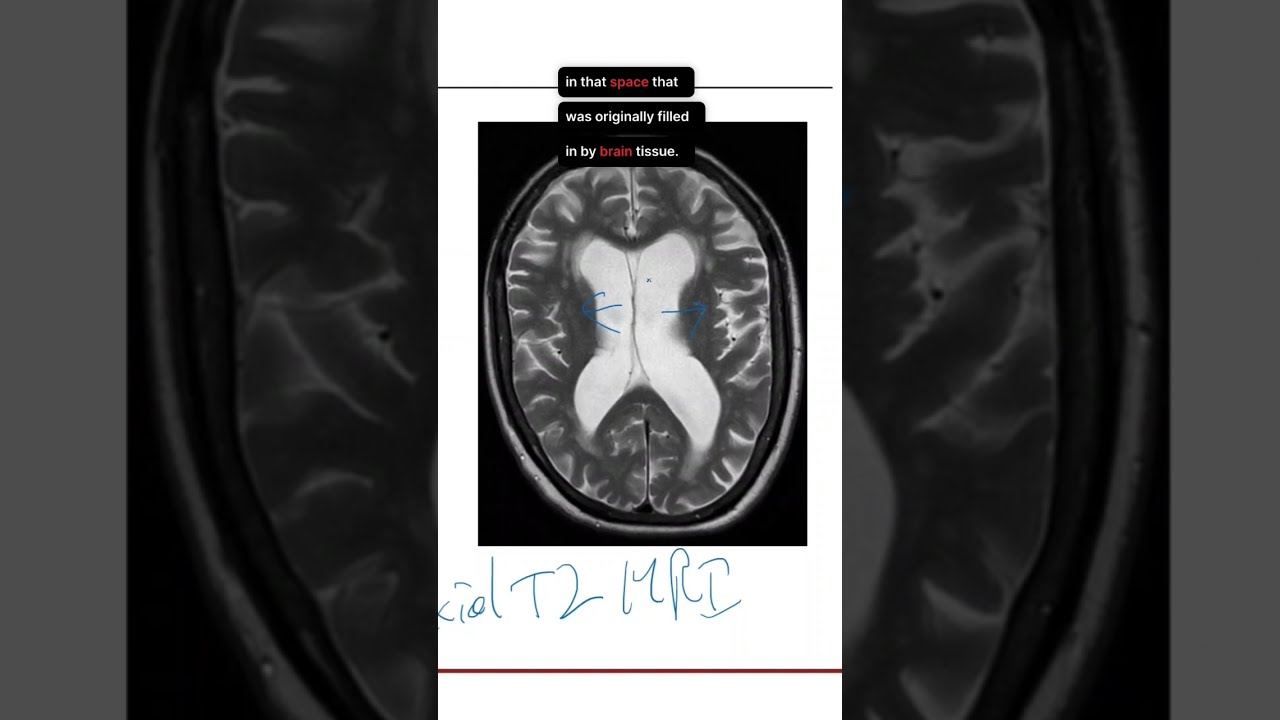
Image taken from the YouTube channel DaVinci Academy Clips , from the video titled Hydrocephalus Ex Vacuo on Brain MRI .
Unveiling the Meaning of Mild Ventriculomegaly Ex Vacuo
Ventriculomegaly, in its simplest definition, refers to the enlargement of the brain’s ventricles, fluid-filled spaces within the brain. A specific type of this condition, ventriculomegaly ex vacuo, is what we will explore in detail.
This article will concentrate specifically on mild to moderate cases of ventriculomegaly ex vacuo, a nuance that significantly shapes its interpretation and management.
The increasing prevalence of this finding in an aging population, coupled with its potential association with cognitive decline, makes understanding it paramount.
Why Understanding Matters
Recognizing and understanding mild ventriculomegaly ex vacuo is increasingly important for several reasons:
-
Aging Population: As the global population ages, age-related brain changes, including cerebral atrophy, become more common.
-
Cognitive Decline: Mild ventriculomegaly ex vacuo is often associated with varying degrees of cognitive impairment or decline, which requires careful assessment and management.
Therefore, distinguishing it from other forms of ventriculomegaly is crucial for proper diagnosis and tailored patient care.
Article Aim
Our aim is to elucidate the meaning and implications of mild to moderate ventriculomegaly ex vacuo.
We aim to provide a comprehensive understanding of this condition.
This will cover its causes, diagnostic evaluation, associated conditions, and management strategies.
Ultimately, this article strives to empower readers with the knowledge necessary to navigate this complex topic and to advocate for the best possible care.
Understanding Ventriculomegaly: More Than Just Enlarged Ventricles
Ventriculomegaly, at its core, describes the enlargement of the brain’s ventricles. These ventricles aren’t just empty spaces; they are a complex network of interconnected cavities located deep within the brain. Understanding their normal function is crucial to grasping the significance of ventriculomegaly, especially when it arises ex vacuo.
The Vital Role of Ventricles and CSF
The ventricles serve as the production and circulation hub for cerebrospinal fluid (CSF). CSF is a clear, colorless fluid that cushions the brain and spinal cord, protecting them from injury.
More importantly, CSF plays a crucial role in removing waste products from the brain and delivering nutrients. Think of it as the brain’s lymphatic system, essential for maintaining a healthy environment.
The constant circulation of CSF through the ventricles, around the brain, and down the spinal cord is critical for optimal brain function. Disruptions to this flow or changes in CSF production or absorption can have significant neurological consequences.
Congenital vs. Acquired Ventriculomegaly: A Key Distinction
Ventriculomegaly can be broadly categorized as either congenital or acquired. Congenital ventriculomegaly is present at birth, often resulting from developmental abnormalities during fetal development. This type can be associated with a range of genetic syndromes or prenatal infections.
Acquired ventriculomegaly, on the other hand, develops later in life.
This can occur due to various factors, including traumatic brain injury, infections, or, as we will discuss, brain atrophy.
The "ex vacuo" type falls under the umbrella of acquired ventriculomegaly. Understanding this distinction is essential because the underlying causes and management strategies differ significantly between congenital and acquired forms.
Ventriculomegaly Ex Vacuo: Enlargement Due to Brain Tissue Loss
As we’ve established, ventriculomegaly simply refers to enlarged ventricles. However, the reason behind that enlargement is critical. When the underlying cause is brain tissue loss, we are dealing with ventriculomegaly ex vacuo.
The Latin phrase "ex vacuo" literally translates to "from emptiness." This term accurately describes the underlying mechanism of this specific type of ventriculomegaly.
Instead of being caused by increased pressure or obstruction of CSF flow, as seen in hydrocephalus, ventriculomegaly ex vacuo arises because the brain tissue surrounding the ventricles has shrunk or atrophied.
Cerebral Atrophy: The Driving Force
Cerebral atrophy, or the loss of brain cells and connections, is the primary driver of ventriculomegaly ex vacuo. As brain tissue diminishes, the ventricles expand to fill the void, similar to how the air space in a deflating balloon increases.
This atrophy can affect the entire brain or be localized to specific regions. The degree of ventricular enlargement generally correlates with the extent and severity of cerebral atrophy.
Several factors can contribute to cerebral atrophy, including:
- Normal aging processes
- Neurodegenerative diseases (Alzheimer’s disease, frontotemporal dementia)
- Vascular events (stroke)
- Chronic traumatic encephalopathy (CTE)
The specific cause of atrophy will influence the pattern and severity of ventricular enlargement.
Ex Vacuo vs. Hydrocephalus: Understanding the Difference
It is crucial to distinguish ventriculomegaly ex vacuo from hydrocephalus. While both conditions involve enlarged ventricles, their underlying mechanisms and clinical implications are vastly different.
Hydrocephalus: A Matter of Pressure
Hydrocephalus is characterized by an active process involving an imbalance in CSF production, flow, or absorption. This leads to a buildup of CSF within the ventricles, causing increased pressure on the surrounding brain tissue.
This increased pressure can damage the brain and lead to a range of neurological symptoms.
Ventriculomegaly Ex Vacuo: Filling a Void
In contrast, ventriculomegaly ex vacuo is a passive process. There is no obstruction to CSF flow, and the pressure within the ventricles is typically normal.
The ventricles simply expand to occupy the space left behind by the atrophied brain tissue.
Put simply, hydrocephalus is akin to a balloon being overfilled with air. Ventriculomegaly ex vacuo is analogous to a balloon partially deflating, with the air expanding to fill the available space.
This distinction is fundamental for proper diagnosis and treatment. While hydrocephalus often requires interventions to relieve pressure, such as a shunt, the primary focus in ventriculomegaly ex vacuo is identifying and addressing the underlying cause of the cerebral atrophy.
Mild to Moderate Ventriculomegaly Ex Vacuo: Defining the Spectrum
As we’ve established that ventriculomegaly ex vacuo arises from the loss of brain tissue, understanding the degree of ventricular enlargement becomes crucial. This section focuses on defining what constitutes "mild" and "moderate" ventriculomegaly ex vacuo, often relying on imaging-based measurements to guide these classifications. The severity is directly linked to the underlying cerebral atrophy, which we will also explore.
Quantifying Ventricular Size
Determining whether ventriculomegaly ex vacuo is mild, moderate, or severe relies heavily on objective measurements obtained from brain imaging, specifically MRI and CT scans. While subjective assessments exist, quantitative metrics provide a more standardized approach.
The Evans’ Index and Other Metrics
One commonly used metric is the Evans’ Index. This index calculates the ratio of the maximum width of the frontal horns of the lateral ventricles to the maximum internal diameter of the skull at the same level. Generally, an Evans’ Index greater than 0.3 suggests ventriculomegaly.
However, it is important to remember that the Evans’ Index is just one tool, and its reliability can vary. Other measurements, such as the ventricular volume and the width of specific regions of the ventricles, may also be considered.
Furthermore, these values should be interpreted in context, taking into account the patient’s age and overall brain health.
Defining Mild vs. Moderate
While precise cut-off values may vary slightly between institutions and depending on the specific measurement used, the following general definitions apply:
-
Mild ventriculomegaly typically involves ventricular enlargement that is subtly beyond the normal range, but not overtly dramatic. The Evans’ Index may be slightly elevated above 0.3, or other measurements might show a modest increase compared to age-matched norms.
-
Moderate ventriculomegaly demonstrates more pronounced ventricular enlargement. The ventricles are clearly larger than expected, and the Evans’ Index may be significantly above 0.3.
It’s essential to recognize that these classifications are not strict categories, but rather points on a spectrum. The distinction between mild and moderate can be somewhat subjective, and clinical judgment is always necessary.
The Atrophy-Ventriculomegaly Connection
Cerebral atrophy is the sine qua non of ventriculomegaly ex vacuo. The degree of ventricular enlargement is directly related to the amount of brain tissue that has been lost. As neurons and their connections diminish, the ventricles expand to fill the resulting space.
Correlation Between Atrophy Severity and Ventriculomegaly Grade
In mild cases, the degree of cerebral atrophy may be subtle and difficult to detect on imaging alone. The ventricles are only slightly enlarged, reflecting a minimal loss of brain volume.
Moderate cases generally indicate more significant cerebral atrophy. Imaging might reveal not only enlarged ventricles, but also widened sulci (the grooves on the brain’s surface) and thinning of the cerebral cortex.
It is crucial to understand that atrophy isn’t always uniform. It may be more pronounced in certain brain regions, leading to asymmetrical ventricular enlargement or disproportionate changes in specific areas.
Common Causes of Cerebral Atrophy
Understanding the etiology of the atrophy is paramount for appropriate management. Cerebral atrophy can stem from a variety of causes, which are especially relevant in the aging population:
-
Normal aging: As we age, some degree of brain tissue loss is expected. This is often a gradual process and may result in mild ventriculomegaly ex vacuo.
-
Neurodegenerative diseases: Conditions like Alzheimer’s disease, frontotemporal dementia, and Parkinson’s disease are characterized by progressive neuronal loss, leading to significant cerebral atrophy and ventriculomegaly.
-
Vascular disease: Strokes or chronic cerebrovascular disease can cause localized or widespread brain damage, resulting in atrophy and ventricular enlargement.
-
Inflammatory and Infectious Diseases: Certain infections of the brain and surrounding tissues may also lead to atrophy.
-
Traumatic Brain Injury: Head trauma can cause brain damage and subsequent atrophy, potentially contributing to ventriculomegaly ex vacuo.
The clinical context, patient history, and specific imaging findings are crucial for determining the underlying cause of cerebral atrophy and the corresponding degree of ventriculomegaly.
Diagnostic Evaluation: Seeing is Believing – Imaging and Assessment
The identification and evaluation of mild to moderate ventriculomegaly ex vacuo rely heavily on a combination of advanced brain imaging techniques and thorough neurological assessments. These tools allow clinicians to visualize the structural changes in the brain, quantify the degree of ventricular enlargement, and assess the patient’s neurological function, ultimately leading to a more informed diagnosis and management plan.
The Indispensable Role of Brain Imaging
Brain imaging is paramount in both diagnosing ventriculomegaly and determining its underlying cause. Magnetic Resonance Imaging (MRI) and Computed Tomography (CT) scans are the primary modalities employed, each offering unique advantages.
MRI is generally preferred due to its superior soft tissue resolution. It provides detailed images of the brain parenchyma, allowing for a more accurate assessment of cerebral atrophy, white matter changes, and the presence of any structural lesions.
CT scans, while offering less detailed soft tissue imaging, are often quicker and more readily available, making them useful in emergency situations or when MRI is contraindicated. They are also excellent for visualizing bone structures and detecting acute bleeds.
Unveiling Brain Structure with Imaging
These imaging techniques provide crucial information about:
-
Ventricular Size: Clearly demonstrating the degree of ventricular enlargement, allowing for the quantification discussed in the previous section.
-
Brain Tissue Volume: Assessing the extent of cerebral atrophy, the hallmark of ventriculomegaly ex vacuo. Imaging can reveal generalized or focal volume loss.
-
Lesions or Abnormalities: Identifying any structural lesions, such as strokes, tumors, or areas of inflammation, that may be contributing to brain atrophy or causing hydrocephalus, which needs to be ruled out.
The Neurological Examination: A Comprehensive Assessment
While imaging provides a structural view of the brain, a comprehensive neurological assessment is essential for evaluating the functional impact of ventriculomegaly and associated brain atrophy.
This involves a detailed evaluation of:
- Motor Function: Assessing strength, coordination, and gait.
- Sensory Function: Testing the patient’s ability to perceive touch, pain, temperature, and vibration.
- Reflexes: Evaluating the integrity of the nervous system pathways.
- Cranial Nerves: Assessing the function of the nerves that control vision, hearing, facial movements, and other vital functions.
Assessing Cognitive Function: A Critical Component
Given the potential association between cerebral atrophy and cognitive decline, a thorough assessment of cognitive function is an indispensable part of the diagnostic process. This often involves the use of standardized neuropsychological tests designed to evaluate various cognitive domains, including:
-
Memory: Assessing both short-term and long-term memory function.
-
Executive Function: Evaluating the ability to plan, organize, and execute tasks.
-
Attention and Concentration: Measuring the ability to focus and maintain attention.
-
Language: Assessing language comprehension and expression.
The results of these tests, combined with the imaging findings and neurological examination, help clinicians determine the extent and nature of any cognitive impairment and guide appropriate management strategies.
Clearly visualizing the brain’s structure and identifying any present abnormalities sets the stage for the next critical step: understanding the underlying causes contributing to the observed ventriculomegaly ex vacuo. Determining the "why" is paramount to formulating an appropriate management strategy.
Underlying Causes and Associated Conditions: Piecing Together the Puzzle
Mild to moderate ventriculomegaly ex vacuo is rarely an isolated finding. It almost always points to an underlying process of brain tissue loss. This section explores the conditions frequently associated with cerebral atrophy and, consequently, this specific type of ventricular enlargement.
The Aging Brain and Ventriculomegaly
Perhaps the most common association is with normal aging.
As we age, our brains naturally undergo changes, including a gradual reduction in volume. This age-related brain atrophy is a common finding on imaging studies of elderly individuals.
While the degree of atrophy varies from person to person, it can often manifest as mild to moderate ventriculomegaly ex vacuo. It is crucial to differentiate this age-related change from more pathological causes.
Neurodegenerative Diseases: A Significant Contributor
Neurodegenerative diseases represent a significant category of underlying causes. These conditions are characterized by the progressive loss of neurons and synaptic connections.
Alzheimer’s Disease
Alzheimer’s disease, the most prevalent form of dementia, is strongly associated with cerebral atrophy, particularly in the temporal and parietal lobes. This atrophy contributes directly to the development of ventriculomegaly ex vacuo.
Frontotemporal Dementia (FTD)
FTD is another neurodegenerative disorder that can cause significant frontal and temporal lobe atrophy. The resulting volume loss can lead to prominent ventricular enlargement.
Parkinson’s Disease and Related Disorders
Parkinson’s disease and related disorders like Lewy Body Dementia can also contribute to cerebral atrophy, although often to a lesser extent than Alzheimer’s or FTD.
Vascular Contributions: Stroke and White Matter Disease
Vascular disease, including stroke and white matter disease, can also lead to cerebral atrophy and ventriculomegaly ex vacuo.
Stroke
A stroke, whether caused by a blood clot or hemorrhage, can result in localized brain damage and subsequent atrophy in the affected area. If the stroke is significant, it can contribute to overall brain volume loss and ventricular enlargement.
White Matter Disease
White matter disease, often seen on MRI as areas of hyperintensity, represents damage to the myelin sheaths that insulate nerve fibers. Severe white matter disease can disrupt neuronal connections and contribute to diffuse cerebral atrophy.
Other Potential Causes of Cerebral Atrophy
While age-related changes, neurodegenerative diseases, and vascular disease are the most common culprits, other conditions can also contribute to cerebral atrophy and ventriculomegaly ex vacuo. These include:
- Traumatic Brain Injury (TBI): Significant TBI can cause widespread brain damage and subsequent atrophy.
- Infections: Certain infections, such as encephalitis or meningitis, can lead to brain tissue loss.
- Inflammatory Conditions: Chronic inflammatory conditions affecting the brain can also contribute to atrophy.
- Substance Abuse: Long-term alcohol or drug abuse can have detrimental effects on brain volume.
It’s important to recognize that the presence of mild to moderate ventriculomegaly ex vacuo should prompt a thorough investigation to identify the underlying cause. This understanding is essential for developing an appropriate and individualized management plan.
Clinical Implications and Management Strategies: Addressing the Underlying Issues
The presence of mild to moderate ventriculomegaly ex vacuo, while often an incidental finding on brain imaging, isn’t without potential consequences. Its true significance lies in what it reveals about the underlying health of the brain. Understanding the potential impact on cognitive function and quality of life is crucial for guiding appropriate management strategies.
Cognitive Impact and Quality of Life
The degree to which ventriculomegaly ex vacuo affects cognitive function and quality of life is highly variable. It depends primarily on the extent and location of the underlying cerebral atrophy.
While mild cases might be asymptomatic or present with only subtle cognitive changes, more pronounced atrophy can lead to noticeable impairments. These impairments can range from mild memory lapses to significant difficulties with executive functions like planning, problem-solving, and decision-making.
These cognitive changes can, in turn, impact daily living activities, social interactions, and overall well-being, affecting a patient’s ability to maintain independence and enjoy a fulfilling life.
Therefore, a comprehensive neuropsychological assessment is often warranted to evaluate the specific cognitive domains affected and the severity of impairment.
Treating the Cause, Not the Symptom
It’s critically important to understand that ventriculomegaly ex vacuo itself is not the target of treatment. It is merely a signpost indicating that something else is happening in the brain.
The primary focus of management should always be on identifying and addressing the root cause of the cerebral atrophy. This requires a thorough evaluation to determine the underlying etiology, whether it’s age-related brain changes, a neurodegenerative disease, vascular disease, or another contributing factor.
Treatment strategies will vary widely depending on the underlying cause.
Management of Neurodegenerative Diseases
In cases of neurodegenerative diseases like Alzheimer’s disease or FTD, treatment focuses on managing symptoms and slowing disease progression. This may involve medications to improve cognitive function, therapies to support daily living skills, and strategies to manage behavioral symptoms.
Vascular Disease Management
If the ventriculomegaly is related to vascular disease or stroke, management may involve strategies to prevent further strokes, such as blood pressure control, cholesterol management, and antiplatelet therapy.
Lifestyle Interventions and Supportive Care
Regardless of the underlying cause, lifestyle interventions can play a significant role in maintaining cognitive function and improving quality of life. These may include:
- Regular physical exercise to improve blood flow to the brain.
- A healthy diet rich in antioxidants and omega-3 fatty acids.
- Cognitive training activities to stimulate the brain and maintain cognitive abilities.
- Social engagement to reduce isolation and promote mental well-being.
Supportive care, including occupational therapy, speech therapy, and counseling, can also be invaluable in helping patients and their families cope with the challenges of cognitive decline.
Individualized Management is Key
Ultimately, the management of mild to moderate ventriculomegaly ex vacuo must be individualized based on a patient’s specific symptoms, imaging findings, and underlying etiology. A multidisciplinary approach involving neurologists, neuropsychologists, geriatricians, and other healthcare professionals is often necessary to develop a comprehensive and effective management plan.
FAQs: Mild Ventriculomegaly Ex Vacuo
Here are some frequently asked questions to help you better understand mild ventriculomegaly ex vacuo.
What exactly is mild ventriculomegaly ex vacuo?
Ventriculomegaly ex vacuo refers to the enlargement of the brain’s ventricles (fluid-filled spaces) due to a loss of brain tissue, not increased fluid pressure. In the case of mild ventriculomegaly, the enlargement is slight. Generally, mild to moderate ventriculomegal is favired exvacuo in nature, meaning that it is due to brain tissue loss.
What causes ventriculomegaly ex vacuo?
It often results from brain atrophy or damage from prior brain injury that may have happened perinatally or during the lifespan, not a blockage of cerebrospinal fluid (CSF). The lost brain volume creates more space within the ventricles.
Is mild ventriculomegaly ex vacuo something to be worried about?
It depends on the underlying cause and the individual. The prognosis varies based on the extent of brain tissue loss and its impact on brain function. It is imperative to be seen by a medical professional to obtain a diagnosis.
How is mild ventriculomegaly ex vacuo typically managed or treated?
There’s no direct treatment for the ventriculomegaly itself since it is a consequence of the brain tissue loss. Management focuses on addressing the underlying cause, if possible, and supporting any associated neurological deficits. In most cases, mild to moderate ventriculomegal is favired exvacuo in nature which in that case means it is monitored.
So, next time you hear about mild to moderate ventriculomegaly is favored ex vacuo in nature, remember it’s often about figuring out why things look a little bigger on the inside. Hopefully, this cleared things up a bit!